Esthetic-functional rehabilitation for severe and widespread dental wear
Go to gallery
Complete esthetic-functional rehabilitation
Go to gallery
Esthetic-functional rehabilitation on severely compromised dentition
Go to gallery
Esthetic-functional rehabilitation for esthetics and dental wear
Go to gallery
Veneers
Ceramic veneers: upper-anterior area for discoloration
Go to gallery
Ceramic veneers: upper-anterior area for misalignment
Go to gallery
Ceramic veneers: upper-anterior area for wide tooth gaps
Go to gallery
Ceramic veneers: upper-anterior area
Go to gallery
Ceramic veneers: severely worn dentition
Go to gallery
Ceramic veneers: anterior sextant with severe wear and agenesis
Go to gallery
Crowns
Ceramic crown on implants: anterior area
Go to gallery
Ceramic crown on anterior tooth
Go to gallery
Ceramic crown on anterior tooth previously treated
Go to gallery
Ceramic crown on implant: anterior tooth
Go to gallery
Ceramic crown on implant: anterior tooth
Go to gallery
Oral surgery and Implant dentistry
Implant placement on the anterior area
Go to gallery
Guided implant surgery
Go to gallery
Dental bleaching
Home dental bleaching with masks
Go to gallery
In-office dental bleaching
Go to gallery
In-office dental bleaching: devitalized tooth
Go to gallery
In-office dental bleaching: devitalized tooth
Go to gallery
In-office dental bleaching: devitalized tooth
Go to gallery
Conservative dentistry
Anterior tooth restoration
Go to gallery
Replacement of amalgam fillings
Go to gallery
Orthodontics
Early orthodontics with palatal expander
Go to gallery
Early orthodontics: malocclusion and tooth crowding
Go to gallery
Corticotomy-facilitated orthodontics
Go to gallery
Pre-prosthetic orthodontics
Go to gallery
Fixed orthodontics on adult patients
Go to gallery
Endodontics
Re-treatment of a previously devitalized tooth
Go to gallery
Vital tooth root canal treatment
Go to gallery
Oral hygiene and prevention
Professional oral hygiene
Go to gallery
Pediatric dentistry
Dental sealants
Go to gallery
Esthetic-functional rehabilitation on implants
1/6: The patient presents severely worn dentition, especially regarding the upper arch, due to night grinding (bruxism) and chemical erosion.
2/6: The dental wear is so severe as to substantially compromise all functional and esthetic aspects.
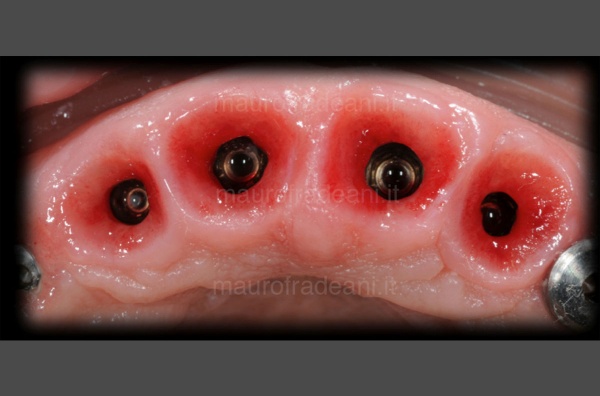
3/6: In order to prosthetically rehabilitate the two arches, it was necessary to extract all the upper teeth and to replace them with osseointegrated implants on which titanium abutments were placed. In the lower arch, on the other hand, the natural teeth were kept and prepared for single full ceramic restorations.
4/6: The lateral view of the final prosthetic rehabilitation shows how function and esthetics have been successfully restored.
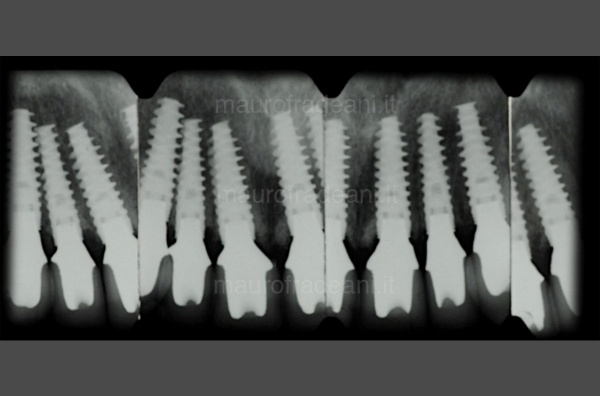
5/6: The X-ray shows the presence of perfectly integrated implants in the upper arch and in the lower right molar. In the rest of the lower arch, the prosthetic restorations were positioned over natural teeth abutments, which were kept vital thanks to minimal dental preparations.
6/6: 6 years later, the prosthetic rehabilitation has been excellently preserved.
Esthetic-functional rehabilitation for severe and widespread dental wear
1/6: Dental abrasion and shortening heavily penalize the young patient's smile.
2/6: With lips parted, no dental portion is exposed, due to reduced tooth lengths. Since this is a peculiar characteristic of elderly patients, the resulting esthetic deficit is particularly evident due to the young age.
3/6: The pre-operative intra-oral view shows the improper tooth inclination, tending towards the inside, as well as a generalized unsatisfactory color of the dentition.
4/6: Intraoral view of the cemented all-ceramic restorations. The esthetic-functional rehabilitation was aimed at re-establishing a correct occlusion, restoring suitable lengths and dental morphologies.
5/6: With lips parted, the patient now exposes an appropriate dental portion suitable to the young age.
6/6: At the end of the treatment, the patient shows a smile fully meeting expectations.
Complete esthetic-functional rehabilitation
1/4: Inadequate shapes, reduced tooth dimensions and unsatisfactory color led the patient to request a prosthetic treatment extended to both arches and aimed at improving esthetics and function.
2/4: Intraoral view before treatment: the esthetic and functional issues exposed by the patient are even more evident.
3/4: Intraoral view of the cemented all-ceramic restorations. Thanks to the esthetic-functional rehabilitation, the correct occlusion was restored by re-establishing suitable lengths and appropriate dental morphologies, as well as a much more pleasant color.
4/4: At the end of the treatment, the restored smile fully meets the patient’s esthetic expectations.
Esthetic-functional rehabilitation on severely compromised dentition
1/4: The patient presents a particularly compromised situation: considerable dental wear, multiple tooth decay and lack of teeth.
2/4: Intraoral view: the patient needs a complete rehabilitation of both arches.
3/4: Intraoral view of the cemented restorations: the esthetic-functional rehabilitation is perfectly integrated in the mouth.
4/4: The picture at the end of the treatment shows a striking change, which gives the patient the confidence of an ideal smile.
Esthetic-functional rehabilitation for esthetics and dental wear
1/4: The patient presents generalized lack of aesthetics in terms of color and alignment, as well as marked dental wear.
2/4: The intraoral view shows inadequate tooth shapes and sizes.
3/4: The aim of this esthetic-functional rehabilitation, involving both arches, was the restoration of suitable tooth shapes and dimensions, while achieving a correct occlusion.
4/4: The final result of the treatment, perfectly integrated in the patient's mouth, fully satisfies all expectations.
Ceramic veneers: upper-anterior area for discoloration
1/9: The intake of tetracyclines has irreparably altered the patient's dental appearance.
2/9: Dental discoloration strongly penalizes the esthetics of the smile.
3/9: The esthetic deficit was solved with a treatment involving ceramic veneers in the upper-anterior area only (from canine to canine).
4/9: Palatal view: the application of restorations is limited to the buccal (external) surface of the teeth.
5/9: Palatal view: the application of restorations is limited to the buccal (external) surface of the teeth.
6/9: Thanks to the use of ceramic veneers, the patient has newly found an ideal dental esthetics.
7/9: Lateral view of the patient’s smile at the end of the treatment.
8/9: Lateral view of the patient’s smile at the end of the treatment.
9/9: The patient's smile shows the remarkable aesthetic improvement at the end of the treatment.
Ceramic veneers: upper-anterior area for misalignment
1/5: The backward position of the lateral incisors compared to the central incisors makes the patient's smile disharmonious.
2/5: An intraoral view further highlights the dental misalignment.
3/5: The esthetic issue can be solved thanks to the application of 2 additive all-ceramic veneers, without having to undergo an orthodontic treatment.
4/5: The intraoral view of the cemented veneers shows the actual esthetic improvement.
5/5: At the end of the treatment, the patient's smile has regained ideal harmonic proportions.
Ceramic veneers: upper-anterior area for wide tooth gaps
1/4: Excessive space and small teeth strongly penalize the patient's esthetic appearance.
2/4: Intraoral view: small teeth and excessive interdental spaces can be noticed.
3/4: The fabrication of 6 ceramic veneers (from canine to canine) of suitable shapes and sizes have led to a significant esthetic improvement thanks to the reduction of spaces between the teeth.
4/4: At the end of the treatment, the patient has regained an esthetically pleasant smile.
Ceramic veneers: upper-anterior area
1/5: The patient wishes to modify the shape of the upper-anterior teeth, which give a disharmonious look to the smile.
2/5: The intraoral view shows an unsatisfactory dental morphology.
3/5: Ceramic veneers are fabricated to correct the esthetic defects.
4/5: Intraoral view of the cemented restorations.
5/5: The appropriate dental shapes make the patient's smile more in line with expectations.
Ceramic veneers: severely worn dentition
1/5: Severe dental wear has significantly reduced the length of the central incisors of this young patient.
2/5: The front teeth before treatment involving ceramic veneers.
3/5: The 4 ceramic restorations, with a thickness of only a few tenths of a millimeter, are ready to be cemented.
4/5: Final picture of the 4 restorations, showing an excellent integration with the surrounding gingival tissues. The esthetic appearance is significantly improved thanks to the new contours, the new proportions and the dominance of the central incisors.
5/5: After 8 years, the restorations show an excellent functional, biological and esthetic integration.
Ceramic veneers: anterior sextant with severe wear and agenesis
1/5: The patient presents congenital agenesis of the right upper lateral incisor and widespread dental wear. The interdental spaces were optimized through orthodontic treatment, before proceeding with the prosthetic treatment with veneers.
2/5: After orthodontically gaining a suitable space, a fixture (osseointegrated implant) was inserted on the site of the missing incisor.
3/5: Before proceeding with the finalization of the restoration, a provisional restoration was positioned on the implant on the upper right lateral incisor, to provide suitable esthetics even in this phase of the treatment.
4/5: At the end of the treatment, the patient has finally gained an ideal smile.
5/5: Frontal view of the restorations: 1 crown on implant on the right lateral incisor and 5 veneers on the remaining anterior teeth.
Ceramic crown on implants: anterior area
1/7: Pre-operative view of the patient’s smile.
2/7: The presence of several infections affecting the anterior teeth has compromised their health state and made extraction necessary.
3/7: Osseointegrated implants were inserted on the site of the extracted teeth, acting as artificial roots for the final restorations.
4/7: The gingival tissues surrounding the implants are modeled according to the shape of the provisional restorations, to idealize the aesthetic result of the final restorations.
5/7: The artificial ceramic (zirconium) abutments are placed on the implants: thanks to its light color, the abutments will ensure an ideal esthetic result of the restoration.
6/7: The final restorations of the anterior area (from canine to canine) show an excellent esthetic, biological and functional integration.
7/7: The smile of the patient at the end of the treatment.
Ceramic crown on anterior tooth
1/2: The upper right central incisor is prepared for the restoration.
2/2: The extremely natural aspect of the restoration makes it perfectly integrated from every esthetic and functional point of view.
Ceramic crown on anterior tooth previously treated
1/5: The young patient presented a clearly inadequate reconstruction of the upper right central incisor.
2/5: The old restoration was anchored to the remaining natural tooth by means of two abutments, which had to necessarily be removed for a correct rehabilitation of the teeth.
3/5: The dental preparation was performed while preserving a suitable amount of enamel to ensure maximum retention of the restoration and thus ensure a good long-term prognosis.
4/5: A close view of the restoration allows to appreciate its natural and perfect esthetic integration.
5/5: At the end of the treatment the patient has finally regained an esthetically pleasant smile.
Ceramic crown on implant: anterior tooth
1/8: The patient presents an inadequate restoration on the left upper central incisor.
2/8: Closer view of the anterior superior sextant. An X-ray examination also reveals the fracture of the root, making it necessary to extract the tooth.
3/8: An osseointegrated implant was inserted on the site of the extracted tooth, acting as an artificial root for the the final restoration.
4/8: An artificial ceramic (zirconium) abutment was placed on the implant: thanks to its light color, the abutment will ensure an ideal esthetic result of the restoration.
5/8: Two different visions of the final restoration (crown), fabricated in all-ceramic.
6/8: The light color of the underlying abutment contributes to the achievement of a highly esthetic result.
7/8: After the cementation, the final restoration looks perfectly integrated from both an esthetic and functional point of view.
8/8: At the end of the treatment, the patient's smile shows a remarkable esthetic improvement.
Ceramic crown on implant: anterior tooth
1/4: The patient presents bone resorption on the upper right central incisor, which has to necessarily be extracted.
2/4: During the extraction, an osseointegrated implant was placed acting as an artificial root for the final restoration.
3/4: An artificial ceramic (zirconium) abutment was placed on the implant: thanks to its light color, the abutment will ensure an ideal esthetic result of the restoration.
4/4: After the cementation, the final restoration looks perfectly integrated from both an esthetic and functional point of view.
Implant placement on the anterior area
1/5: The right lateral incisor, fractured due to dental trauma, must necessarily be extracted.
2/5: The X-ray highlights the fracture of the right lateral incisor.
3/5: The fractured tooth is extracted and replaced by an osseointegrated titanium implant, acting as an artificial root on which the all-ceramic crown will be placed.
4/5: An artificial abutment is placed on the osseointegrated implant; its light color allows to achieve a highly esthetic result.
5/5: At the end of the treatment, the all-ceramic restoration placed on the implant is perfectly integrated from an esthetic, biological and functional point of view.
Guided implant surgery
1/7: The patient's smile shows an excessive exposition of gingiva, and the previous restorations are completely inadequate from an esthetic and functional point of view.
2/7: The intraoral view highlights the inadequacy of the previous prosthetic rehabilitation on both arches: the precarious abutments and crowns will have to be completely removed.
3/7: The pre-treatment X-ray shows a widespread problem of bone loss and the inadequacy of the previous prosthetic restorations.
4/7: The natural teeth are extracted and replaced by osseointegrated titanium implants, on which the artificial ceramic abutments are positioned. Its light color allows to achieve a highly esthetic result.
5/7: The new esthetic restorations fixed to the osseointegrated implants looks perfectly coherent from an esthetic and functional point of view.
6/7: After 12 years, the X-ray shows how the osseointegrated implants and the prostheses are perfectly maintained.
7/7: At the end of the treatment, the patient’s smile no longer shows an excessive part of gingiva, and looks definitely better from an esthetic and functional point of view.
Home dental bleaching with masks
1/4: Unsatisfied with the color of the teeth, the patient would like a brighter smile; with a home whitening treatment, an appreciable result can be reached within a few days.
2/4: The transparent masks, made of acetate fiber, are fabricated from the impressions taken on the patient's dental arches.
3/4: After filling them with whitening gel, the masks have to be worn at night.
4/4: At the end of the treatment, the patient's smile shows a significant improvement in brightness and color of the teeth.
In-office dental bleaching
1/2: The patient requests overall dental whitening to improve the aesthetics of the smile.
2/2: The treatment, which required only two appointments in the office, gave the patient an esthetically satisfying smile.
In-office dental bleaching: devitalized tooth
1/2: A devitalization incorrectly performed years before caused discoloration of the right upper central tooth.
2/2: Tooth root whitening is performed in-office; a small hole is made on the tooth surface, in which the whitening product is inserted.
The result reached after a few sessions shows a clear improvement if compared to the initial situation.
In-office dental bleaching: devitalized tooth
1/2: The tooth shows a remarkable discoloration, caused by an improper devitalization performed long before.
2/2: Tooth root whitening is performed in-office; a small hole is made on the tooth surface, in which the whitening product is inserted.
The result reached after a few sessions shows a clear improvement.
In-office dental bleaching: devitalized tooth
1/4: The left upper central is remarkably darker than the other dental elements, creating discomfort and dissatisfaction in the patient, who would like to harmonise the color of the smile.
Moreover, the reduced length of the right upper central tooth increases the patient's sense of unease.
2/4:
3/4: Thanks to the root whitening of the left central tooth and the restoration of the right central tooth in composite material, the esthetic appearance of the smile is significantly improved.
4/4: At the end of the treatment, the patient shows a remarkably harmonious and esthetically satisfying smile.
Anterior tooth restoration
1/2: A severe trauma resulted in the fracture of a large portion of the left upper central incisor.
2/2: Together with the patient, the clinician decided to use composite material for this extensive restoration. Only one session is needed for this type of operation. The esthetic result achieved is particularly satisfactory.
Replacement of amalgam fillings
1/4: In cases of tooth decay infiltration under old dental amalgam fillings, it is necessary to replace them with composite material which, in addition to a greater biocompatibility, guarantees ideal esthetic results.
2/4: Due to the toxicity of the mercury it contains, the removal of the amalgam must be carried out safely, protecting the patient with special devices such as the rubber dam which, while guaranteeing the isolation of the operating field, allows to have an ideal control of all the materials removed as well as the fluids inside the oral cavity.
3/4: Removing the old filling exposes the decayed dental tissue, which is carefully removed.
4/4: Together with a greater biocompatibility, the composite offers an ideal esthetics to the treated teeth as it perfectly blends with the dental enamel.
Early orthodontics with palatal expander
1/7: Initial picture before early orthodontic treatment. This young patient presents a contraction of the upper jaw and anterior open bite. The upper arch appears therefore “narrower” and “backwards” compared to its ideal position.
2/7: From the lateral view of the arches it is evident that, due to the contraction of the upper jaw, the tooth development would not guarantee the correct "covering" of the upper incisors with regards to the lower ones when the arches are in contact.
3/7: From the lateral view of the arches it is evident that, due to the contraction of the upper jaw, the tooth development would not guarantee the correct "covering" of the upper incisors with regards to the lower ones when the arches are in contact.
4/7: Once positioned, the device (Rapid Palatal Expander - RPE) has to be manually activated once a day for a successful result.
5/7: The right lateral view at the end of the treatment shows how a correct occlusal relationship between the arches has been reached. The enlarged upper arch now correctly occludes with the lower one.
6/7: The left lateral view at the end of the treatment shows how a correct occlusal relationship between the arches has been reached. The enlarged upper arch now correctly occludes with the lower one.
7/7: Picture taken at the end of the treatment: the palate was enlarged with a resultant upper jaw advancement, now correctly occluding with the lower arch.
Early orthodontics: malocclusion and tooth crowding
1/6: Initial picture taken before early orthodontic treatment. The young patient presents a first class malocclusion with misalignment and dental crowding in both arches. The upper right central incisor is in reverse bite with the lower one.
2/6: Upper occlusal picture showing the misalignment of the upper central incisors.
3/6: Lower occlusal picture showing the dental crowding on the lower arch.
4/6: The right lateral view shows the backward position of the upper right central incisor, which determines the incorrect occlusion with the lower arch.
5/6: Right lateral view picture showing the correct position of the upper right central incisor at the end of the orthodontic treatment.
6/6: Front view at the end of the orthodontic treatment: both the misalignment and the initial dental crowding have been fixed.
Corticotomy-facilitated orthodontics
1/3: Initial frontal view picture. The young patient presents severe dental crowding, which would require the extraction of 2 upper and 2 lower premolars to be solved.
2/3: Corticotomy is a small surgical incision of the most superficial layer of the bone reducing its resistance to the orthodontic forces of braces, while exploiting the weakness of the bone during the healing process to accelerate the movement of teeth.
3/3: Front view at the end of the orthodontic treatment. The use of corticotomy made it possible to solve the problem of dental crowding in a much shorter time and, above all, without having to extract any of the premolars.
Pre-prosthetic orthodontics
1/5: The patient presents severe dental crowding with misalignment of the lower incisors, dental shape and volume alteration with enamel wear of the gingival collars and worn incisal margins causing esthetic and functional issues. Before treating this case with prosthetic restorations, a preventive orthodontic realignment is necessary.
2/5:
3/5:
4/5:
5/5:
Fixed orthodontics on adult patients
1/7: The patient presents an inverse occlusal relationship: the lower arch is in an advanced position compared to the upper one.
2/7: The reversed occlusal relationship is even more evident from the side view.
3/7: The orthodontic treatment resulted in the forward movement of the upper arch teeth and the backward movement of the lower arch teeth.
4/7: The lateral view picture, taken after the removal of the braces, allows to analyze the correct re- establishment of a physiological occlusion.
5/7: The smile of the patient before the orthodontic treament.
6/7: At the end of the treatment, the patient's smile has significantly improved also from an esthetic point of view.
7/7: As well as solving the occlusal problem, the orthodontic treatment has given back the patient a greater harmony of the smile.
Re-treatment of a previously devitalized tooth
1/2: Despite already having devitalized the tooth, the patient presents tooth pain and feels gum swelling; a new root canal therapy is therefore necessary.
2/2: The post-operative X-ray shows an adequate root canal therapy, solving all symptoms previously reported by the patient.
Vital tooth root canal treatment
1/2: The patient presents severe pain and a swollen cheek sensation; the X-ray shows an apical lesion (the dark shadow under the root) of the first lower left molar. A Root canal therapy to devitalize the tooth is necessary.
2/2: The X-ray taken 6 months after the surgery shows a marked improvement in the dark area under the root, which has now disappeared. The symptoms complained of by the patient have never occurred again.
Professional oral hygiene
1/2: The accumulation of plaque causes inflammation of the gingival tissues with redness and bleeding, even spontaneous.
2/2: After attending in-office dental hygiene sessions and being taught the right techniques for home oral care, the patient has come back to the clinic with a considerable improvement in the plaque control and restored tissue health.
Dental sealants
1/3: The presence of deep grooves on the teeth surface makes its cleaning difficult and enhances bacterial growth, leading to an increasing risk of tooth decay. The sealing of permanent teeth is a preventive treatment which isolates the grooved and creates a barrier against bacteria.
2/3: This quick and painless operation does not require anesthesia. The treated tooth has to be isolated with a rubber dam preventing contamination.
3/3: The dental sealant, applied with a brush, is a special white-transparent resin with continuous release of fluoride ions. This material guarantees enamel protection for several years and can be newly applied in case of damage.
Contact Dr. Fradeani’s Clinic
Message sent!
We're sorry but an error has occurres. Try to send the form again, if the problem persists write to: info@maurofradeani.it